Internal Limiting Membrane Removal in the Management of Full-Thickness Macular Holes
Viktória Mester, MD1
Ferenc Kuhn, MD, PhD1,2
See below for Figures, Tables and References.
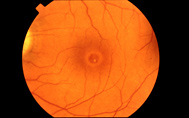 Pre-op Macula Hole |
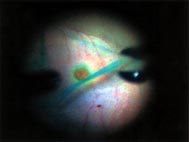 Intra-op Macular Hole |
 Post-op Macular Hole Repair |
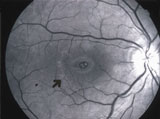
 Post-op Macular Hole Repair |
Abstract
Purpose
To determine the effectiveness of internal limiting membrane (ILM) removal in the treatment of full-thickness macular holes.
Methods
Data were reviewed from a prospective study on 47 consecutive eyes with full-thickness macular holes undergoing vitrectomy, internal limiting membrane maculorhexis, and fluid-gas exchange. No eye underwent repeat macular hole surgery. A meta-analysis was performed to compare the outcomes of different surgical techniques in the treatment of full-thickness macular holes.
Results
The outcome measures were disappearance of the submacular fluid and the change in best-corrected visual acuity. The surgery was anatomically successful in 96% of the eyes and 85% of the eyes showed an improvement of at least two Snellen lines. Best-corrected final vision was =20/40 in 39% of eyes. No permanent complications specifically due to the removal of the macular ILM were detected; the minor hemorrhages and retinal edema seen in most eyes resolved spontaneously. Retinal detachment developed and was successfully treated in three eyes (7%). A meta-analysis on 1701 eyes from published reports showed that ILM maculorhexis appears to significantly (p<0.0001) increase the anatomical and functional success rates in macular hole surgery.
Conclusions
ILM removal is an important development in the evolving field of macular hole surgery. A randomized, prospective, multicenter clinical trial should be performed to determine which surgical technique is the most beneficial in patients with full-thickness macular holes.
1 Department of Ophthalmology, University of Pécs, Hungary
2 Helen Keller Eye Research Foundation, Birmingham, Alabama, U.S.A.
Presented at the Biannual Meeting of the European Society of Ophthalmology in Stockholm, Sweden, June 1999
The study was performed at the Department of Ophthalmology, University of Pécs, Hungary
None of the authors has a propriety interest in the study material.
Corresponding author: Ferenc Kuhn, MD
P.O.Box 55687
Birmingham, Alabama 35255-5687
(205) 558-2588 (tel)
(205) 933-1341 (fax)
It is estimated that idiopathic macular holes involve 33 of every 10,000 individuals over the age of 55.1 Although usually only a minimal amount of fluid accumulates under the fovea, the condition can lead to severe visual impairment and until the early 1990s effective treatment was unavailable. The rationale for surgery originates in traction being identified as the cause of hole formation,2,3 further supported by the finding that misplacement, rather than loss, of the foveal tissue is responsible for the visual deterioration.2,4
The first article reporting on the results of vitrectomy for hole closure was published in 1991.5 The results have greatly improved since,6-10 proving that skepticism is no longer warranted: vitrectomy is superior to observation even for longstanding holes.11-14 The surgical technique varies. Many surgeons use some type of adjuvant to create a permanent seal at the hole’s edge,6-8,10,15-21 while others prefer not to use adjuvants.5,9,12,14,22-30 We report the results of our prospective series of 47 consecutive eyes with idiopathic full-thickness macular holes. No adjuvant was used in any eye, and all eyes underwent complete vitrectomy, removal of the macular internal limiting membrane (ILM), and 30% SF6 implantation with face-down positioning.
Patients and Methods
Included in this prospective series were eyes that developed a full-thickness macular hole with a best-corrected preoperative visual acuity equal to or worse than 20/50. All pre- and postoperative examinations were performed by the two surgeons, and the following criteria were monitored: age and sex of the patient; stage of hole; duration of visual complaints; best-corrected preoperative visual acuity; presence and stage of cataract; presence of posterior vitreous detachment; presence of an epimacular membrane; other notable conditions or characteristics of the eye; intraoperative complications; length of follow-up; postoperative complications including cataract progression/development; additional surgeries; anatomical outcome; best-corrected postoperative visual acuity. Anatomical success was defined as complete disappearance of the subretinal fluid and flattening of the hole’s edge. Functional success was defined as visual acuity improvement of at least two Snellen lines.
The preoperative evaluation included, among others, taking of an extensive history, determination of the Snellen visual acuity, indirect ophthalmoscopy without scleral indentation, and a thorough slit lamp examination using a three-mirror contact lens and/or a 90 diopter lens. A detailed informed consent was obtained in every case.
All surgeries were done at a major university hospital. A standard three-port pars plana vitrectomy was performed, usually under local anesthesia with sedation. Following limited removal of the central vitreous (“reverse sequence vitrectomy;” Kuhn and Mester, unpublished data), we used the vitrectomy probe (Microvit, Alcon Surgical, Fort Worth, Texas) to elevate the posterior hyaloid face at the optic disc. Once the posterior hyaloid face was engaged, we carefully enlarged the detachment in a circular motion. Separation of the hyaloid from the retina was confirmed by the appearance of the Weiss ring and by the advancing, concentric demarcation line between areas of the ILM covered by, and free of, vitreous. Frequently, the edge of the macular hole temporarily elevated as the vitreous from around the hole was removed; the hole’s edge collapsed back as the anterio-posterior traction was relieved.
After completing the vitrectomy, we removed all epiretinal membranes. If the patient was awake, he/she was repeatedly warned to avoid any head or body movement before manipulations over the macular area were to be performed.
With a disposable blade, previously tipped against a metal surface to form a small hook at an angle of approximately 70 degrees, we created an opening in the ILM in the macular area, always outside the maculopapillary bundle. The direction of the incision typically followed the natural course of the nerve fibers. If a hemorrhage developed along the incision or grabbing of the ILM edge was unsuccessful, the incision was repeated elsewhere.
We used a forceps (Storz [St. Louis, Missouri] #65410) to grasp the ILM (see Table 1 for differential diagnosis between ILM and an epimacular membrane). The ILM was not always easy to visualize, especially in elderly patients. Once caught and elevated, the ILM became easier to recognize due to its characteristic light reflex. In very young and elderly patients with idiopathic holes (as opposed to middle aged individuals and those with traumatic holes), the ILM was usually fragile. If it tore, we had to reengage the edge of the sometimes still adherent ILM. To identify the ILM’s edge, we used as guidance the different light reflexes from the ILM-free and ILM-covered retinas. A normal shine was seen over the attached ILM, as opposed to the dull reflex seen over the area denuded of the ILM. Also helpful was the pale color of the retina in the area of ILM removal.
The ILM was carefully elevated using the forceps as a spatula for blunt dissection; as the forceps was advanced, we paid careful attention to maintain the instrument’s tip in the proper plane. The ILM was torn in a circular motion, similar to that seen during creation of a capsulorhexis. Infrequently and mostly in young patients, the ILM was strongly adherent in certain areas, making it difficult and potentially dangerous to continue the rhexis. In such cases, we excised the ILM around the adherence. In one eye the ILM was firmly adherent at the hole’s margin and we performed radial cuts rather than forced the peeling. This eye was one of the anatomical failures. Typically, half of the ILM was torn in a clockwise and the other half in a counterclockwise motion; we avoided monodirectional dialing for convenience and safety.
The ILM was usually removed from an area extending to the vascular arcades. The lifting and tearing required only minimal force; if the ILM prematurely tore, it was removed in several pieces rather than as one large sheet. To avoid enlargement of the hole, special attention was paid to peel the ILM towards, and never from, the macular hole. We did not attempt to drain the subretinal fluid through the hole.
After the retinal periphery was examined for breaks, an air-fluid exchange was performed. The intraocular pressure never exceeded 25 mm Hg at the end of wound closure. Using a 30 gauge needle, approximately 1,6 ml air was withdrawn from the midvitreous, and an equal amount of SF6 gas was injected. Longer-acting gases were not used. At the conclusion of surgery, each patient received one drop of timolol as well as subconjunctival antibiotics and corticosteroids, always injected away from the sclerotomy sites.
Each patient was asked to position face-down for up to 10 days, but compliance was questionable in several cases. The gas was reinjected in cases of too early absorption.
Although the ILM was unmistakably and verifiably removed in all of the 47 eyes, for further confirmation we sent several specimens to undergo laboratory investigations such as light microscopy, transmission (Figs. 1 and 2) and scanning electron microscopy, and antibodies against type IV collagen.
Results
In this prospective series of 47 consecutive eyes with full-thickness macular holes, 11 of the 47 patients (23%) were males. The ages ranged from 13 to 78 years (average, 50 years); 23% were younger than 60 years. All complained of decreased, and approximately half of them also of distorted, vision. Duration of the visual complaints was known in 38 patients (81%). The hole existed for an average of 5 (1 to 26) months. Six eyes (13%) were pseudophakic, 12 (26%) had cataract preoperatively, and two patients (4%) had a macular hole in the fellow eye. The hole was idiopathic in 91% of the eyes and trauma-related in four eyes. Preoperative visual acuities ranged from count fingers to 20/50.
Few intraoperative complications were encountered. Small capillary hemorrhages were typical as the ILM was incised or lifted. The hemorrhage was more substantial in five eyes (11%), but in only one case was it necessary to temporarily raise the intraocular pressure. In most eyes we noticed that the area freed from the ILM became somewhat opaque, signifying a mild retinal edema. The hemorrhages and the edema disappeared by the next day from every eye.
The average follow-up was 11 (3-27) months; the median was also 7 months. One patient was lost and 37% of eyes had a follow-up exceeding a year. Surgery was anatomically successful in 44 of the 46 eyes (96%, Figs. 3 and 4). Postoperative visual acuities ranged from 20/300 to 20/20. The vision improved at least two lines in 39 eyes (85%) and at least three Snellen lines in 35 eyes (76%). The average and median improvements were 4 Snellen lines with 39% of eyes reaching =20/40 best-corrected vision. Of the seven functional failures, the vision was unchanged in three eyes (7%) and improved one line in four (9%). In four eyes the SF6 gas had to be reinjected, but no reoperation for macular hole was performed.
Postoperatively, retinal detachment developed and was successfully treated in three eyes (7%). The preexistent cataract progressed in five eyes (11%); in 13 eyes (28%) cataract development was noted. To date 13 eyes (28%) underwent cataract extraction with intraocular lens implantation. Reproliferation in the area of ILM removal has not been detected, nor have we seen retinal damage from the endoscopic light.
Light microscopy, electron microscopy, and antibodies against type IV collagen verified that the removed specimens were indeed consistent with the ILM. Clinically, the absent light reflex in the ILM-denuded area is pathognomic.
Discussion
The original surgical technique to close idiopathic macular holes involved a complete vitrectomy and stripping of all epiretinal membranes.5 A variety of adjuvants have been also been advocated,6-8,10,15-21,27,28,31-38 two of which in the initial studies promised significant improvement. However, transforming growth factor-beta 2 in a prospective, randomized, double-masked, placebo-controlled clinical trial has not been found beneficial,28 and the early enthusiasm regarding the use of autologous blood has also subsided as in later series its efficacy could not be confirmed.16,31,39 Complications such as severe inflammation,40 endophthalmitis,41 proliferative vitreoretinopathy,19 and retinal hemorrhages42 are more common with adjuvants. The considerable cost involved40 also justified the search for an alternative.
In the largest series to date published on vitrectomy for Terson’s syndrome,43 we found that in 39% of the eyes a hemorrhagic cyst developed at the macula. Of these cysts, 69% were submembranous, i.e., the blood accumulated under the ILM. We removed the ILM in all eyes and followed some patients closely for over eight years, finding no clinically visible reproliferation. Vision improved to 20/25 or greater in 83% of the eyes.44 We suggested in 1994 that intentional ILM removal should be considered for traction maculopathies such as macular holes45 and have peeled the ILM for macular holes since the mid 1990s.
Newly formed collagen and glial cells, macrophages, myofibroblasts, fibrocytes, retinal pigment epithelial cells, and fibrous astrocytes are responsible for the tangential traction.46-48 These cells have been identified on both sides of the ILM,46,48 its wrinkling49-51 supporting the ILM’s role in the development of tangential traction.49,52 Such traction, originating in the acellular prefoveal vitreous, appears to be the initial cause of hole formation; hole enlargement is due to myofibroblastic contraction on the ILM.48,51,53 Idiopathic, full-thickness macular holes can form in the presence of well-documented, preexisting complete posterior vitreous detachment,52 and macular hole formation and epimacular proliferation have been suggested to have a common pathogenesis.47 These findings support the concept of ILM removal and the clinical experience regarding its efficacy in macular hole surgery.29,30,37
Adjuvant use may not be necessary in macular hole surgery if the ILM is removed. There is no reason to presume that macular holes behave differently from breaks intentionally created during submacular surgery.39 Such breaks close and remain closed without adjuvant use or laser retinopexy; should all traction around the hole be eliminated, a macular hole should also be able to seal.54
Removal of the still adherent macular ILM is not an easy surgical procedure. In addition to the technique we described (“ILM maculorhexis,” a term coined by R. Morris, MD, involves mechanical stripping of the still attached ILM in a fashion similar to that seen in forceps-removal of the anterior lens capsule), ILM can also be accomplished by direct grabbing.29 A new technique called FILMS (fluidic internal limiting membrane separation55 promises easier and more atraumatic dissection of the ILM: a foot-driven pump is used to inject 20 µg of Healon (Pharmacia, Uppsala, Sweden) under the ILM, simulating events during the formation of a hemorrhagic macular cyst in Terson’s syndrome.
Removal of the ILM does not appear to lead to specific complications. With appropriate precautions, light toxicity from the fiberoptics can be eliminated.56 Minor hemorrhages and mild, temporary retinal edema commonly occur, but no author found ILM peeling-related damage to the nerve fibers.29,37,48 While several studies reported on the development of visual field defects following macular hole surgery in up to 17% of eyes,25,57-60 the ILM was not removed in these series. The field defects appear to be fluid-gas exchange-related59-61 with dehydration of the nerve fibers possibly playing a key role.62 Use of humidified air may be of prophylactic value (Ohji, M. et al, IOVS 39:S834, 1998). A study on 123 eyes with ILM removal did not find temporal field defects.30
The peripheral retinal breaks, occurring in up to 19% of eyes,37,63,64 are the consequence of surgical posterior vitreous face detachment. Retinal detachment develops in up to 14% of eyes undergoing macular hole surgery.37,64 Retinal detachment was seen in three eyes (7%) in this series; a vigorous examination of the periphery before fluid-gas exchange must be carried out to reduce the incidence of peripheral retinal breaks. The surgeon should also be vigilant to remove the lens if it hinders visualization. In one of our retinal detachment cases we noted that while the cataract permitted perfect viewing of the posterior pole, the lower periphery could not be visualized. The detachment originated from an inferior break. Prophylactic indirect ophthalmoscopic laser cerclage (Morris and Kuhn, British Journal of Ophthalmology, accepted for publication) may reduce the incidence of retinal detachment.
Intraocular gas tamponade plays an important role in postvitrectomy cataract formation or progression (83% in one series14). It is conceivable that a shorter gas tamponade is sufficient if the is ILM peeled. We could not, however, prove this hypothesis.
Different series from the literature are difficult to compare because the variables are not standardized. Until a prospective, randomized, double-masked clinical trial is performed, a meta-analysis with a sufficiently large number of cases offers the only method to determine whether a new surgical procedure is worthwhile to pursue. Because of its severe limitations, however, a meta-analysis should be interpreted only with extreme caution. Table 2 shows the characteristics of 12 published studies in which the traditional technique was used: epiretinal membrane peeling, no adjuvant. The overall anatomical success rate among the 708 cases was 77%, the functional 55%. Using various types of adjuvants in 22 series (Table 3), the overall anatomical success rate among the 772 cases was 81%, the functional 60%. In the four studies with ILM peeling but no adjuvant use (Table 4), the overall anatomical success rate among the 221 cases was 96%, the functional 81% (98 eyes). Using Fisher’s two-sided exact test, ILM maculorhexis appears to significantly (p<0.0001) increase both the anatomical and functional success rates.
Macular hole surgery is still evolving. Removal of the ILM is increasingly accepted as a reasonable alternative to the traditional technique or to adjuvant use.37,48 It is encouraging that in this series with ILM maculorhexis no eye had worse postoperative than preoperative vision. Since the follow-up time in 63% of our cases was shorter than a year, we can reasonably expect further improvement with time.65 As there are few published cases of ILM peeling, a prospective, randomized, double-masked, multicenter study, and not the results of a meta-analysis, should determine whether the apparent 15%-20% increase in the success rate as compared to other techniques is indeed verifiable.
Acknowledgement:
The authors wish to thank Hans E. Grossniklaus, MD (Emory Eye Center, Atlanta, GA), for evaluating the histologic specimens and Richard Maisiak, PhD, MSPH (School of Medicine, University of Alabama at Birmingham), for the statistical analyses.
Table 1. Differentiating between and managing an epiretinal membrane (ERM) versus the internal limiting membrane (ILM)
| ERM | ILM | |
| Appearance | Opaque, nonreflective, semitransparent, soft, irregular surface/border/thickness | Clear, reflective, transparent, elastic, regular surface, no border, thickness increases toward disc |
| When removed | More than one layer possible, reduced adherence to retina, varies with age and individual | Single layer, mild to strong adherence to retina (individual variability that is not necessarily age-related) |
| How to start | If free edge: forceps; if no free edge: forceps, blade, or scraper | Blade; forceps; special cannula;55 never with scraper 66 |
| Where to start | At free edge and/or where convenient | Away from hole, outside maculopapillary bundle and preferably not over retinal vessel |
| Peeling direction | As convenient | Toward fovea, parallel with nerve fibers; never from hole |
| Peeling technique | As convenient | Blunt ILM separation recommended; use spatula (“ILM separator”, Synergetics [St. Louis, Missouri] #20.01) or forceps. Single swift tearing impossible; halfway through procedure tearing should stop and remaining ILM half be approached from opposite direction; consider radial excision/s if peeling at the hole’s edge impossible |
| Ease of removal | Usually easy | May be very difficult, even after edge is found |
Table 2. Literature review: Macular hole surgery without adjuvant use or internal limiting membrane peeling
| First author, year, reference | # of eyes | Stage of hole | Gas used | Adjuvant used | 1Anatomic success (%)2Functional success (%) |
| Thompson 1998 28 | 57 | 2-4 | 16% PFC | None | 61 40 |
| Minihan 1997 27 | 20 | 2-4 | 20% SF 6 | None | 75 55 |
| Freeman 1997 14 | 59 | 3-4 | 16% PFC | None | 69 19 |
| Smiddy 1997 26 | 43 | 2-4 | 16% PFC | None | 91 65 3 |
| Pendergast 1996 25 | 50 | 2-4 | •30% SF 6 or •20% PFC | None 4 | 88 56 |
| Willis 1996 9 | 132 | 2-4 | 40% SF 6 | None | 91 73 |
| Ruby 1994 24 | 33 | 2 | Non-expanding gas | None | 67 5 61 |
| Ryan 1994 23 | 68 | 2-4 | 16% PFC or •24% SF 6 | None | 71 65 |
| Wendel 1993 22 | 170 | 3-4 | Typically SF 6 | None | 77 56 |
| Orellana 1993 12 | 12 | 3 | 20% SF 6 | None | 58 58 |
| Kelly 199 5 | 52 | 3-4 | Non-expanding gas | None | 58 42 |
| Total | 708 | 77 55 |
SF6 = sulfur hexafluoride; PFC = perfluorocarbon (perfluoropropane or perfluoroethane);
1 with one surgery and defined as disappearance of the fluid cuff; 2 defined as an improvement of two or more Snellen lines; 3 •3 Snellen lines; 4 in 14% of eyes = autologous serum was used; 5 anatomic success defined as “closed or smaller” hole.
Table 3. Literature review: Adjuvant use in macular hole surgery; no internal limiting membrane peeling
| First author, year, reference | # of eyes |
Stage of hole | Gas used | Adjuvant used | 1Anatomic success (%)2Functional success (%) |
| McCuen 1999 38 | 40 | 2-4 |
–
|
Silicone oil | 80 58 |
| Olsen 1998 37 | 24 | 2-4 | 10% PFC | Autologous cryoprecipitate, bovine thrombin | 96 NA |
| Thompson 199828 | 63 | 2-4 | 16% PFC | TGF-ß2 | 78 48 |
| Peyman 1997 36 | 19 | 3-4 | Air/nonex-panding gas | Gelatin plug | 100 59 |
| Minihan 1997 27 | 15 | 2-4 | 20% SF6 | TFG-ß2 | 67 33 |
| Minihan 1997 27 | 50 | 2-4 | 16% PFC | Autologous platelet cc | 96 73 |
| Kusaka 1997 35 | 29 | 2-4 | 16% PFC | Autologous serum | 97 76 |
| Gaudric 1997 34 | 77 | 2-4 | 17% PFC | Autologous platelet cc | 93 NA |
| Kozy 1996 33 | 17 | Persistent holes | •16% PFC | TGF-ß2 | 94 71 |
| Polk 1996 32 | 71 | 2-4 | 16% PFC | TGF-ß2 | 85 82 |
| Vine 1996 18 | 25 | 2-4 | 10% PFC | Thrombin | 80 68 |
| Liggett 1996 31 | 62 | 3-4 | NA | Autologous serum | 92 NA |
| Wells 1996 16 | 43 | 2-4 | 16% PFC, 30% SF6 | Autologous serum | 67 49 |
| Mori 1996 7 | 14 | 2-4 | NA | Autologous serum | 86 79 |
| Korobelnik 199620 | 8 | 3-4 | 15% PFC | Autologous platelet cc | 86 50 |
| Liggett 1995 8 | 11 | 3-4 | 16% PFC | Autologous serum | 100 100 |
| Gaudric 1995 6 | 20 | 2-4 | 17% PFC | Autologous platelet cc | 95 85 |
| Iwasaki 1995 21 | 26 | NA | NA | Fibrin adhesive | 85 73 |
| Blumenkrantz 1994 17 | 26 | 3-4 | PFC | Autologous plasma, thrombin | 77 NA |
| Tilanus 1994 19 | 15 | 3-4 | 16% PFC | Tissucol glue | 87 53 |
| Lansing 1993 10 | 24 | 2-4 | NA | TFG-ß2 | 96 85 |
| Glaser 1992 15 | 58 | 2-4 | 16% PFC | TGF- ß2 | 64 43 |
| Total | 737 | 81 60 |
SF6 = sulfur hexafluoride; PFC = perfluorocarbon (perfluoropropane or perfluoroethane); cc = concentrate; NA = datum not provided or impossible to interpret; TFG-ß2 = transforming growth factor-beta 2 (bovine, porcine, recombinant, or human); 1 with one surgery and defined as disappearance of the fluid cuff; 2 defined as an improvement of two or more Snellen lines.
Table 4. Literature review: Internal limiting membrane peeling in macular hole surgery with no adjuvant use
| First author, year, reference | # of eyes |
Stage of hole | Gas used |
Adjuvant used
|
1Anatomic success (%)2Functional success (%) |
| Mester 1999 | 46 | 2-4 | •40% SF6 | None | 96 85 |
| Rice 1999 30 | 123 | 2-4 | None | 98 NA | |
| 3Olsen 1998 37 | 13 | 2-4 | NA | None | 92 77 |
| Eckardt 1997 29 | 39 | 2-4 | 20% PFP | None | 92 77 |
| Total | 221 | 96 81 |
SF6 = sulfur hexafluoride; PFP = perfluoropropane; NA = datum not provided or impossible to interpret; 1 with one surgery and defined as disappearance of the fluid cuff; 2 defined as an improvement of two or more Snellen lines; 3 only those eyes with idiopathic macular holes are included.
Figures
 |
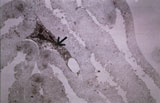 |
| Figure 1. Typical electronmicroscopic appearance of an ILM specimen removed during macular hole surgery. Note the redundant ribbon of the ILM with a smooth inner (arrow) and a rough (arrowhead) surface. | Figure 2. A cell (arrow) sitting on the inner ILM surface, causing contraction of the membrane. |
 |
 |
| Figure 3. Preoperative picture of a stage 2 macular hole. Note the shiny appearance of the ILM in the area temporal to the fovea (arrow). | Figure 4. Postoperative picture of the eye shown on Figure 3. The hole is closed, the submacular fluid has resolved. Note that the light reflex seen on Figure 3 is not visible and the posterior pole has rather dull appearance as the ILM was removed in this area. |
References
- Freeman, W.: Vitrectomy surgery for full-thickness macular holes. Am J Ophthalmol 1993;116:233-235.
- Gass, J.: Reappraisal of biomicroscopic classification of stages of development of macular hole. Am J Ophthalmol 1995;119:752-759.
- Johnson, R. Gass, J.: Idiopathic macular holes: observations, stages of formation, and implications for surgical intervention. Ophthalmology 1988;95:917-924.
- Madreperla, S., McCuen, B., Hickingbotham, D. Green, W.: Clinicopathologic correlation of surgically removed macular hole opercula. Am J Ophthalmol 1995;120:197-207.
- Kelly, N. Wendel, R.: Vitreous surgery for idiopathic macular holes. Arch Ophthalmol 1991;109:654-659.
- Gaudric, A., Massin, P., Paques, M., Santiago, P., Guez, J., Le Gargasson, J., Mundler, O. Drouet, L.: Autologous platelet concentrate for the treatment of full-thickness macular holes. Graefe’s Arch Clin Exp Ophthalmol 1995;233:549-554.
- Mori, K., Yoneya, S. Abe, T.: Vitrectomy with autoserum for idiopathic macular hole. Acta Societatis Ophthalmologicae Japonicae 1996;100:458-463.
- Liggett, P., Skolik, S., Horio, B., Saito, Y., Alfaro, V. Mieler, W.: Human autologous serum for the treatment of full-thickness macular holes. Ophthalmology 1995;102:1071-1076.
- Willis, A. Garcia-Cosio, J.: Macular hole surgery. Ophthalmology 1996;103:1811-1814.
- Lansing, M., Glaser, B., Liss, H., Hanham, A., Thompson, J., Sjaarda, R. Gordon, A.: The effect of pars plana vitrectomy and transforming growth factor-beta 2 without epiretinal membrane peeling on full-thickness macular hole. Ophthalmology 1993;100:868-872.
- Fine, S.: Vitreous surgery for macular hole in perspective. Arch Ophthalmol 1991;109:635-636.
- Orellana, J. Liebermann, R.: Stage III macular hole surgery. Br J Ophthalmol 1993;77:555-558.
- Roth, D., Smiddy, W. Feuer, W.: Vitreous surgery for chronic macular holes. Ophthalmology 1997;104:2047-2052.
- Freeman, W., Azen, S., Kim, J., el-Haig, W., Mishell, D. Bailey, I.: Vitrectomy for the treatment of full-thickness stage 3 or 4 macular holes. Arch Ophthalmol 1997;115:11-21.
-
Glaser, B., Michels, R., Kuppermann, B., Sjaarda, R. Pena, R.: Transforming growth factor-beta 2 for the treatment of full-thickness macular holes. Ophthalmology 1992;99:1162-1173.
- Wells, J. Gregor, J.: Surgical treatment of full-thickness macular holes using autologous serum. Eye 1996;10:593-599.
- Blumenkranz, M., Coll, G., Chang, S. Morse, L.: Use of autologous plasma-thrombin mixture as adjuvant therapy for macular hole. Ophthalmology 1994;101:S69.
- Vine, A. Johnson, M.: Thrombin in the management of full-thickness macular holes. Retina 1996;16:474-478.
- Tilanus, M. Deutman, A.: Full-thickness macular holes treated with vitrectomy and tissue glue. Int Ophthalmol 1995;18:355-358.
- Korobelnik, J., Hannouche, D., Belayachi, N., Branger, M., Guez, J. E. T. Hoand-Xuan, T.: Autologous platelet concentrate as an adjunct in macular hole healing: a pilot study. Ophthalmology 1996;103:590-594.
- Iwasaki, T., Sanada, A., Yamamoto, K., Okada, A. Usui, M.: The use of fibrin tissue adhesive in the treatment of macular holes. Invest Ophthalmol Vis Sci 1995;36:S1050.
- Wendel, R., Patel, A., Kelly, N., Salzano, T., Wells, J. Novack, G.: Vitreous surgery for macular holes. Ophthalmology 1993;100:1671-1676.
- Ryan, E. Gilbert, H.: Results of surgical treatment of recent-onset full-thickness idiopathic macular holes. Arch Ophthalmol 1994;112:1545-1553.
- Ruby, A., Williams, D., Grand, M., Thomas, M., Meredith, T., Boniuk, I. Olk, R.: Pars plana vitrectomy for treatment of sgae 2 macular holes. Arch Ophthalmol 1994;112:359-364.
- Pendergast, S. McCuen, B. I.: Visual field loss after macular hole surgery. Ophthalmology 1996;103:1069-1077.
- Smiddy, W., Pimentel, S. Williams, G.: Macular hole surgery without using adjunctive additives. Ophthalmic Surg Lasers 1997;28:713-717.
- Minihan, M., Goggin, M. Cleary, P.: Surgical management of macular holes: results using gas tamponade alone, or in combination with autologuos platelet concentrate, or transforming growth factor ß2. Br J Ophthalmol 1997;81:1073-1079.
- Thompson, J., Smiddy, W., Williams, G., Sjaarda, R., Flynn, H., Margherio, R. Abrams, G.: Comparison of recombinant transforming growth factor beta-2 and placebo as an adjunctive agent for macular hole surgery. Ophthalmology 1998;105:700-706.
- Eckardt, C., Eckardt, U., Groos, S., Luciano, L. Reale, E.: Entfernung der Membrana limitans interna bei Makulalochern. Klinische und morphologische Befunde. Ophthalmologe 1997;94:545-551.
- Rice, T.: Internal limiting membrane removal in surgery for full-thickness macular holes. Boston, Butterworth Heinemann, 1999, pp. 125-146.
- Liggett, P.: Success with macular hole surgery. Ophthalmology 1996;103:201.
- Polk, T., Smiddy, W. Flynn, H.: Bilateral visual function after macular hole surgery. Ophthalmology 1996;103:422-426.
- Kozy, D. Meberley, A.: Closure of persistent macular holes with human recombinant transforming growth factor-ß2. Can J Ophthalmol 1996;31:179-182.
- Gaudric, A., Paques, M., Massin, P., Santiago, P. Dosquet, C.: Use of autologous platelet concentrate in macular hole surgery: report of 77 cases. Dev Ophthalmol 1997;29:30-35.
- Kusaka, S., Sakagama, K., Kutsuna, N. Ohashi, Y.: Treatment of full-thickness macular holes with autologous serum. Jpn J Ophthalmol 1997;41:332-338.
- Peyman, G., Daun, N., Greve, M., Yang, D., Wafapoor, H. Rifai, A.: Surgical closure of macular hole using an absorbable macular plug. Int Ophthalmol 1997;21:81-97.
- Olsen, T., Sternberg, P. J., Capone, A. J., Martin, D., Grossniklaus, H. Aaberg, T. S.: Macular hole surgery using thrombin-activated fibrinogen and selective removal of the internal limiting membrane. Retina 1998;18:322-329.
- McCuen, B. I., Goldbaum, M. Hanneken, A.: Silicone oil in the treatment of idiopathic macular holes. Boston, Butterworth Heinemann, 1999, pp. 147-154.
- Melberg, N. Mereditg, T.: Success with macular hole surgery. Ophthalmology 1996;103:201.
- Olsen, T., Sternberg, P. J., Martin, D., Capone, A. J., Lim, J. Aaberg, T.: Postoperative hypopyon after intravitreal bovine thrombin for macular hole surgery. Am J Ophthalmol 1996;121:575-577.
- Cohen, S., Hammer, M. Grizzard, W.: Endophthalmitis after pars plana vitrectomy with or without autologous blood products for macular hole. Ophthalmology 1996;103:161.
- Fekrat, S., Wendel, R., Cruz, Z. Green, R.: Clinicopathologic correlation of an epiretinal membrane associated with a recurrent macular hole. Retina 1995;15:53-57.
- Kuhn, F., Morris, R., Mester, V. Witherspoon, C. D.: Terson’s syndrome. Results of vitrectomy and the significance of vitreous hemorrhage in patients with subarachnoid hemorrhage. Ophthalmology 1998;105:472-477.
- Morris, R., Kuhn, F., Witherspoon, C. D., Mester, V. Dooner, J.: Hemorrhagic macular cysts in Terson’s syndrome and its implications for macular surgery. Basel, Karger, 1997, pp. 44-54.
- Morris, R., Kuhn, F. Witherspoon, C. D.: Retinal folds and hemorrhagic macular cysts in Terson’s syndrome. Ophthalmology 1994;101:1.
- Heidenkummer, H. Kampik, A.: Morphologische Analyse epiretinaler Membranen bei chirurgisch behandelten idiopathischen Makulaforamina. Licht-und elektronenmikroskopische Ergebnisse. Ophthalmologe 1996;93:675-679.
- Messmer, E., Heidenkummer, H. Kampik, A.: Ultrastucture of epiretinal membranes associated with macular holes. Graefe’s Arch Clin Exp Ophthalmol 1998;236:248-254.
- Yoon, H., Brooks, H., Capone, A., L’Hernault, N. Grossniklaus, H.: Ultrastructural features of tissue removed during idiopathic macular hole surgery. Am J Ophthalmol 1996;122:67-75.
- Akiba, J., Ishiko, S., Hikichi, S., Ogasawara, T., Yanagia, N. Yoshida, A.: Imaging of epiretinal membranes in macular holes by scanning laser ophthalmoscopy. Am J Ophthalmol 1996;121:177-180.
- Gass, J.: Idiopathic senile macular hole. Arch Ophthalmol 1988;106:629-639.
- Guyer, D., Green, W., de Bustros, S. Fine, S.: Histopathologic features of idiopathic macular holes and cysts. Ophthalmology 1990;97:1045-1051.
- Gordon, L., Glaser, B., Thompson, J. Sjaarda, R.: Full-thickness macular hole formation in eyes with a pre-existing complete posterior vitreous detachment. Ophthalmology 1995;102:1702-1705.
- Smiddy, W., Michels, R., de Bustros, S., de la Cruz, Z. Green, W.: Histopathology of tissue removed during vitrectomy for impending idiopathic macular holes. Am J Ophthalmol 1989;108:360-364.
- Berger, J. Brucker, A.: The magnitude of the bubble buoyant pressure: Implications for macular hole surgery. Retina 1998;18:84-86.
- Morris, R. Kuhn, F.: Surgical treatment of macular surface disorders. Panama City, Highlights of Ophthalmology International, 1998, pp. 58-64.
- Kuhn, F., Morris, R. Massey, M.: Photic retinal injury from endoillumination during vitrectomy. Am J Ophthalmol 1991;111:42-46.
- Hutton, W., Fuller, D., Snyder, W., Fellman, R. Swanson, W.: Visual field defects after macular hole surgery. Ophthalmology 1996;103:2152-2159.
- Ezra, E., Arden, G., Riordan-Eva, P., Aylward, G. Gregor, Z.: Visual field loss following vitrectomy for stage 2 and 3 macular holes. Br J Ophthalmol 1996;80:519-525.
- Boldt, H., Munden, P., Folk, J. Mehaffey, M.: Visual field defects after macular hole surgery. Am J Ophthalmol 1996;122:371-381.
- Kerrison, J., Haller, J., Elman, M. Miller, N.: Visual field loss following vitreous surgery. Arch Ophthalmol 1996;114:564-569.
- Yan, H., Dhurjon, L., Chow, D., Williams, D. Chen, J.: Visual field defect after pars plana vitrectomy. Ophthalmology 1998;105:1612-1616.
- Welch, J.: Dehydration injury as a possible cause of visual defect after pars plana vitrectomy for macular hole. Am J Ophthalmol 1997;124:698-699.
- Sjaarda, R., Glaser, B., Thompson, J., Murphy, R. Hanham, A.: Distribution of iatrogenic retinal breaks in macular hole surgery. Ophthalmology 1995;102:1387-1392.
- Park, S., Marcus, D., Duker, J., Pesavento, R., Topping, P., Frederick, A. D’Amico, D.: Posterior segment complications after vitrectomy for macular hole. Ophthalmology 1995;102:775-781.
- Leonard, R., Smiddy, W., Flynn, H. Feuer, W.: Long-term visual outcomes in patients with successful macular hole surgery. Ophthalmology 1997;104:1648-1652.
- Kuhn, F., Mester, V. Berta, A.: The Tano diamond dusted membrane scraper: indications and contraindications. Acta Ophthalmol 1998;76:754-756.
